Blood gases.

What is the normal range of Ph in an arterial blood gas?
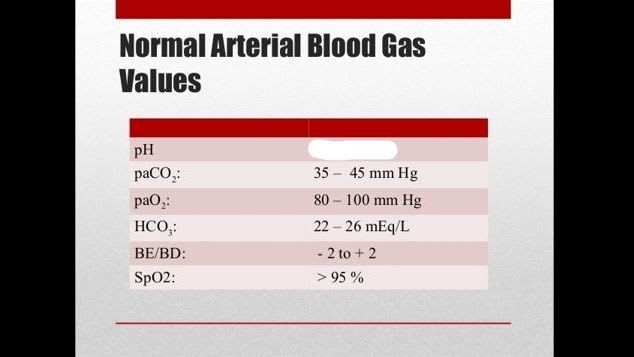
Lower than a Ph of 6.8 or higher than 7.8 is generally not considered compatible with life. However there are occasional case reports of people surviving a Ph of 6.53 (eg 65yr old lady in shock with a splenic artery rupture that was ligated and a splenectomy performed ---BMJ case report 2013).
A persons Pa02 decreases with advancing age. What formula can you use to approximate what the Pa02 should be adapted for age?

Now that is a face with character---sure not many teeth, but a lot of character.
After looking at the Ph to see whether the patient is acidotic or alkalotic what next parameter do you look at to see if the problem is primarily respiratory or metabolic?
Say the patient is acidotic---if the C02 is elevated the primary problem is respiratory if the C02 is lowered it is metabolic.
Conversely
Say the patient is alkalotic--if the C02 is elevated the primary problem is metabolic if it is lowered t is respiratory.
A 25yr old lady presents to ED distressed following the death of a friend. What does the blood gas show?
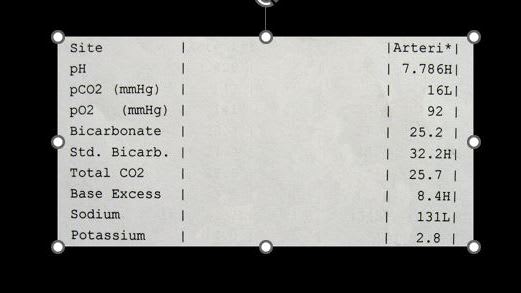
The lady is hyperventilating. Because it is acute the kidneys have not had time to compensate. They would compensate by peeing out HC03 to oppose the alkalosis.
Off handedly this would be about 2mEQ/L of HC03 for every 10mmHg drop in PaC02.
Most people forget that equation after exams.
Mr Creosote is overweight, with poor eating habits and has obstructive sleep apnoea. Which of the following arterial blood gases would be consistent with his appearance at the start of the meal?
Mr Creosote will have chronic respiratory problems. His PaC02 is chronically elevated. Because of this the kidneys compensate by holding back HC03 to keep the Ph in the normal range.
Kidney (renal) compensation is 4 Meq/l for every 10mmHg the C02 is chronically elevated. (This equation is kind of worth remembering).
A 24yr old man was involved in a motorbike crash and has a flail chest. He is saturating 90% on 6l O2 via a Hudson mask. Which of the following ABGs is most likely to be his?
The flail chest has given him acute respiratory acidosis as he is unable to get rid of C02. Acutely the drop in Ph is 0.08 x (the patients C02 -40).
He also not surprisingly has low Pa02 despite being on 02 supplementation.
A 14yr old girl presents with Diabetic Ketoacidosis. This is her ABG . Ph 7.10 PaC02 18 Pa02 94 HC03 4. What does it show?

The ketoacids in diabetic ketoacidosis gives us the metabolic acidosis (in this case severe). The body responds by hyperventilating in order to "blow off" C02 (thus the PaC02 is low). This hyperventilation response however has not brought the Ph back up to normal so the respiratory compensation is called "incomplete".
A 10 day old boy presents with projectile vomiting. He is diagnosed as having pyloric stenosis. What would you expect his blood gas to show?

When the baby vomits in pyloric stenosis he vomits up HCL and K from the stomach. Losing H+ gives him an alkalosis. The body compensates by hypoventilating allowing the C02 to rise.
The kidneys also respond to the baby vomiting up Cl by holding back HC03---so the HC03 is elevated.
What does the mnemonic MUDPILES refer to?

If a patient has a metabolic acidosis you can see whether they have an increased anion gap. That is, add the Na (major cation) and minus the Cl and HC03 (anions). Normally this is about 8 to 16 mEq/L.
If it is greater than this then you have an increased anion gap metabolic acidosis and can use the MUDPILES mneumonic to look for a cause. (google it--as I don't have the room to go through all the causes in MUDPILES).
Different animals have different coloured blood. Which of the following is a lie?

Leeches have yellow blood. In the case of the octopus it has heamocyanin that uses copper instead of iron to bind oxygen so their oxygenated blood is blue.