Aortic dissection.

In an aortic dissection which layer of the aortic wall does the dissection rip along?
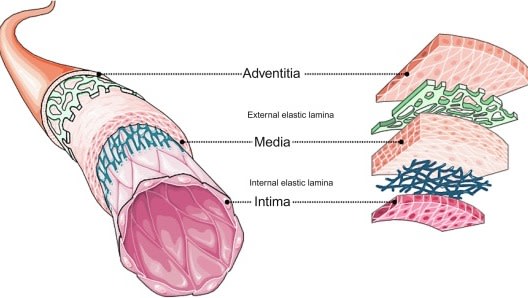
After breaking through the Tunica intima the blood rips through the "middle layer"or Tunica media. PS the Tunica albuginea is below the waist.
Which of the following is INCORRECT about the Stanford Classification of aortic dissections?
The DeBakey classification has l, ll , lll. In l just the ascending aorta is involved. In ll just the descending aorta is involved. In lll both the ascending and descending aorta are involved. I think most people use the Stanford Classification.
How often do patients complain of pain when they present to the ED with a dissection?

Always a bit surprising that it is not higher. Percentage is from Aldeen et al 2009; IRAD data. I suppose it is good to remember that very occasionally the patient may not complain of pain.
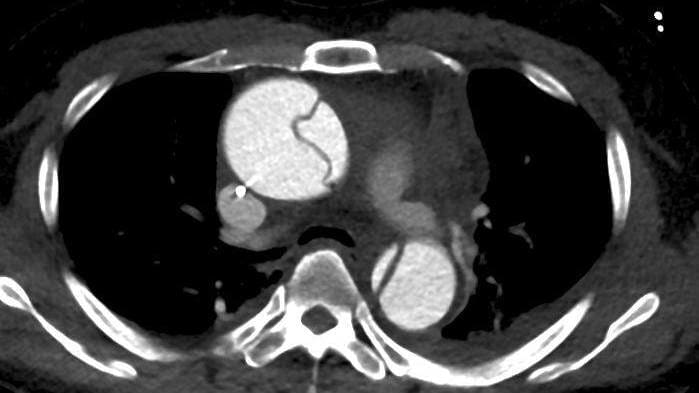
The patient has presented with ripping chest pain going through to the back. This is the CT which does not show a dissection. Why is this?

You can just make out a line across the descending aorta. IV contrast would have easily shown the dissection.
All of these people had an aortic dissection. Which one had their dissection treated against their wishes?
Debakey (in his 90s) developed a dissection and declined an OT despite what his colleagues wanted. As he lost consciousness they decided to do it anyway--he survived.
Which of these conditions does NOT increase your chance of developing an aortic dissection?
Men have about double the risk of developing an aortic dissection compared to women.
This patient is writhing in pain and you strongly suspect an aortic dissection. This is his ECG. What do you do?
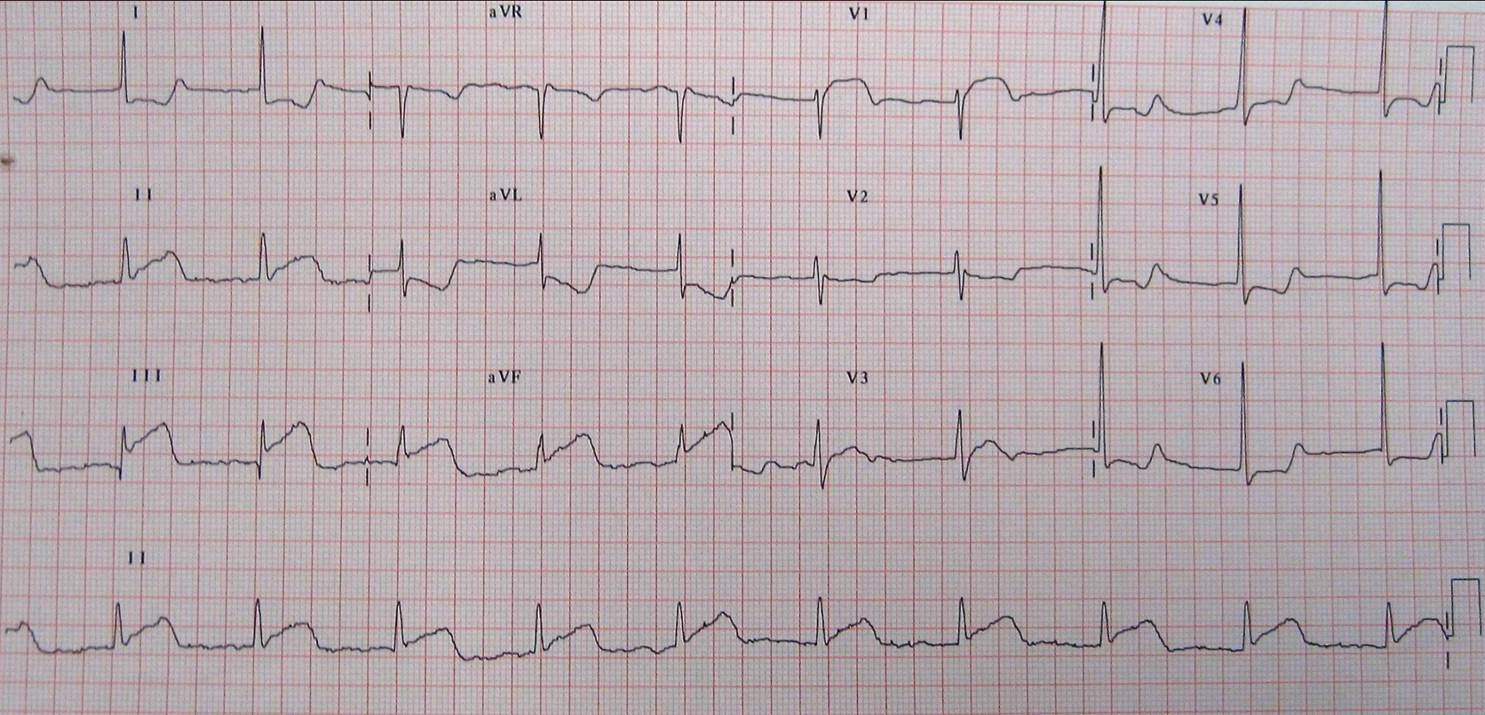
Occasionally in a dissection involving the ascending aorta it can dissect into the right coronary artery as seen here (as the RCA and LCA come off the aorta). If you suspect it you need to do the definitive investigation ASAP which is a CTA.
What symptoms are not recognised as being caused by an aortic dissection?

There are many symptoms, often neurological associated with obstruction of flow in aortic branches by the dissection. If a patient has chest/back pain and a neurological symptom---think dissection.
This patient has a Type A dissection. His BP is 190/90, pulse 98/min and pain 9/10. What would you do to decrease his pain?
You are looking to decrease the heart rate to 60/min then the BP to ideally 120 systolic. Pain will decrease with the drop of heart rate and BP. Fentanyl is useful as a relatively cardiovascularly safe narcotic. MgS04 has no role. GTN is OK but can cause a reflex tachycardia.
This is a PLAX view of the heart. What does it show?
You can sometimes see a Type A dissection in the PLAX, supra sternal and Apical 5 chamber views.