Abdominal trauma.

What imaging is required in this patient with an isolated stab to the abdomen?

An obvious deep stab wound. Simply needs to go to OT not waste time in ED. All the imaging mentioned will not change management.
The video is part of an EFAST examination of a man who suffered a fall from a horse and is hypotensive. What does it show?
There is a large amount of free fluid. No obvious injury to the liver is seen in this short video. Given the history he most likely has ruptured his spleen.
Which of the following best describes this CT of a man who fell off a ladder onto his left side?
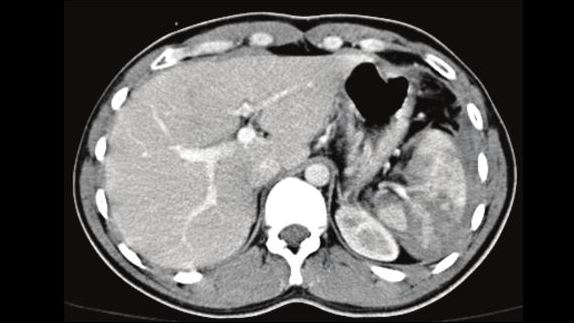
There is a AAST (American Association for the Surgery of Trauma) classification of splenic injuries from I to V. Essentially I is a < 1cm lac or capsular haematoma up to a V being a shattered spleen. This is a IV. Below is a radiopaedia link that fleshes it out.
https://radiopaedia.org/articles/aast-spleen-injury-scale?lang=us
The CT shows a ruptured left kidney. Which of the following statements about blunt trauma to the kidney is INCORRECT.

CT is the preferred imaging modality. Very occasionaly (eg avulsions of the vascular pedicle, Grade 5 injuries) a nephrectomy is performed but generally the treatment of blunt trauma injuries of the kidney is conservative.
Which famous man was thought to have died from a punch to his abdomen which precipitated a ruptured appendix?

Harry Houdini always boasted that he had powerful abdominal muscles and could take any punch if braced. A University student punched him 4 times and he died a number of days later from a rupture of the appendix. The punch is thought to have caused the rupture.
What role does DPL have in blunt abdominal trauma in Sydney today.

With the widespread use of FAST and higher sensitivities of CT I cannot see a role for DPL in Sydney today. If FAST is negative and CT doesnt show anything but you are concerned for a small bowel or mesenteric injury---go to OT and have a look.
(Feel free to contact me and debate its role)
What abdominal injury should you be especially concerned about if your patient has a "Chance" fracture?

Chance fractures can occur in seatbelt injuries. Although of course any intrabdominal organ could be injured you need to especially think about duodenal and pancreatic injuries.
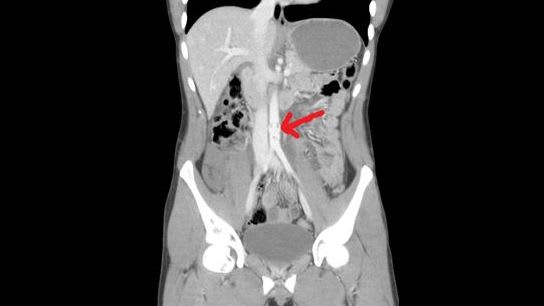
This CT shows radiological signs of a small bowel perforation. How accurate are CTs in picking up bowel perforations in trauma?

So----not perfect but pretty good.
Of the people who get to hospital alive after blunt trauma what percentage are found to have abdominal aortic injuries?
Very uncommon. Essentially I suppose if you rupture your aorta from blunt or penetrating injury you are stuffed. Only the dissections or contained haematomas could make it to hospital.
What is thought to happen when you get "winded".
A truly horrible feeling after you land on your back or front. Sitting in a crouch position is meant to assist the diaphragm to relax.