Oncological Emergencies.
A man is 9 days post chemotherapy and has a temperature of 39 degrees. He is suspected of having febrile neutropenia. Which of the following responses is best practise?
You have to assume he is neutropenic and commence antibiotics ASAP. Tazocin 4.5gm IV is a good option (Note--it has Piperacellin in it which is a Penicillin--- so do not give if the patient is allergic to Penicillins---in which case Ceftazadime 2gm IV would be an option).
Which of the following statements is INCORRECT about "Leukostasis"?
It may affect any organ but most commonly affects the lungs and brain. Overall acute onset of dyspnoea is the most common presentation.
This sign can occur in patients with SVC obstruction. What is it called?
Named after the now deceased Hugh Pemberton. It means the patient has a thoracic inlet obstruction and was initially described in a patient with a large retrosternal goitre.
The video shows a patient with pericardial tamponade caused by a malignancy. Which malignancy most commonly causes this?
The video shows RV and RA diastolic collapse as well as a distended IVC. The patient unsurprisingly required urgent pericardial drainage.
Why is the chemotherapy agent "Adriamycin" (doxorubicin) nicknamed the "Red Devil"?

It does have a broad group of side effects including very occasionally causing dilative cardiomyopathy.
Hypercalcemia occurs in 10 to 30% of patients with cancer. In terms of the initial care in ED which therapy is the most important to initiate?

These patients are inevitably dehydrated. The most effective initial treatment is to get them rehydrated. The other options may all become part of your treatment regime but IV fluids is your first line in ED.
Tumour lysis syndrome occurs when there is the breakdown of a large number of malignant cells which spills their contents into the circulation. Which of the following statements summarises the subsequent problems best?
The broken cells spill out K and Phosporus (which binds to Ca to cause CaPO4--and therefore cause low free Calcium). They also spill out nucleic acids which are broken down to uric acid which in turn causes acute kidney injury.
This MRI (from radiopaedia) shows spinal cord compression from a metastasis Which of the following statements about metastatic spinal cord compression is INCORRECT?

These patients need early recognition, early steroids and early involvement of oncology and neurosurgery.
Hyperviscosity syndrome occurs most commonly in diseases with high paraproteins in the blood but can occur in leukemia. What is the classic triad of symptoms?

Classically it occurs in Waldenstrom macroglobuliemia but can occur if you have very high white cells (Leukemia), Red cells (Polycythemia), Platelets (Thrombocytosis) or other high paraproteins (Myeloma). The problem is "thick blood" which obstructs vessels and buggers up platelet function (thats why the bleeding occurs).
What is generally recognised as the first chemotherapy drug?
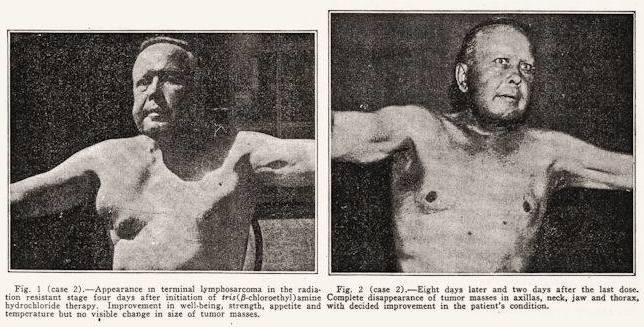
In 1942 Goodman and Gilman noted the effects of Mustard Gas to cause lymphoid and myeloid suppression. They altered the compound and created Nitrogen mustard. The photo is of their first patient. This is a link to a Wikepedia page that briefly tells the unusual story. https://en.wikipedia.org/wiki/Nitrogen_mustard