Heart blocks.
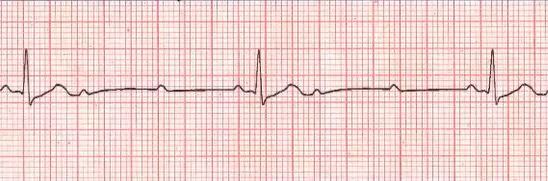
What does this short rhythm strip show?
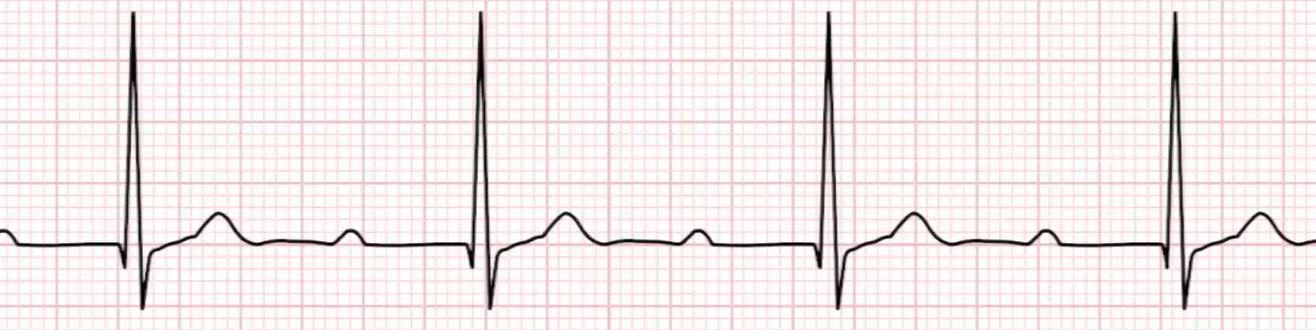
The PR interval is prolonged (> 5 small squares) but that prolongation is the same with every beat.
This patient was in CCU following an inferior AMI. What does this rhythm strip show?

Mobitz type 1 is also called Wenkebach just to confuse and annoy everyone. The PR interval stretches from beat to beat then you get a dropped beat and the whole thing starts over again. The number of beats the PR interval stretches before dropping a beat varies from patient to patient--it may be 3 to 1, 4 to 1 etc.
The following ECG was an incidental finding on an elderly gentleman pre operatively. What does it show?
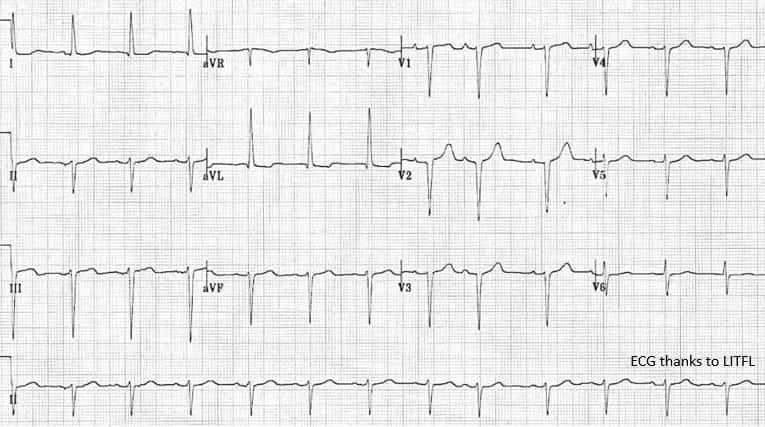
You can see left axis deviation. Small r and big s waves in the inferior leads (ll,lll,aVF) as well as small q big R wave in lateral leads (l,aVL).
if this gentleman had coronary artery disease it is a predictor of total and cardiac mortality. However if he does not have known CAD it is of little or no prognostic significance.
This elderly man presented to ED with a collapse. What does the ECG show?
There is complete dissociation between the P waves and QRS complexes. The ventricle is "escaping" at a rate of about 20/min. No wonder he collapsed.
What does this rhythm strip show?
There is consistently 2 P waves that do not conduct. The 3rd always conducts and its PR interval is constant. So it is Mobitz type 2.
What does this ECG show?

Sinus rhythm. Left axis deviation. Broad QRS, Downward deflected QRS V1. Notched R wave lateral leads with t wave inversion---------LBBB.
Use Sgarbossa criteria (do what I do when I forget and google it) if the patient has a LBBB and you think they may have suffered a myocardial infarct.
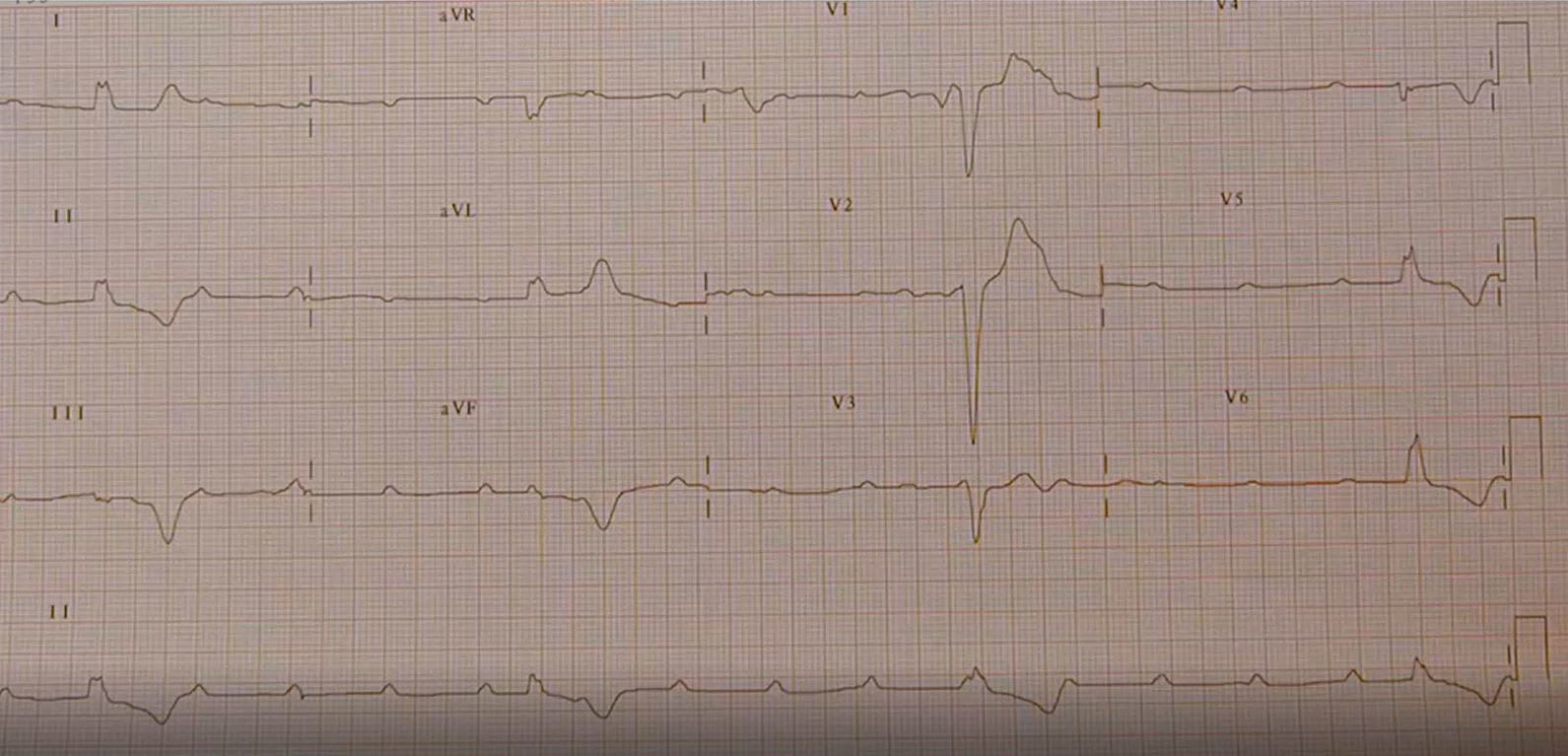
A 72yr old has a history of coronary artery disease and presents with chest tightness. What does the ECG show?
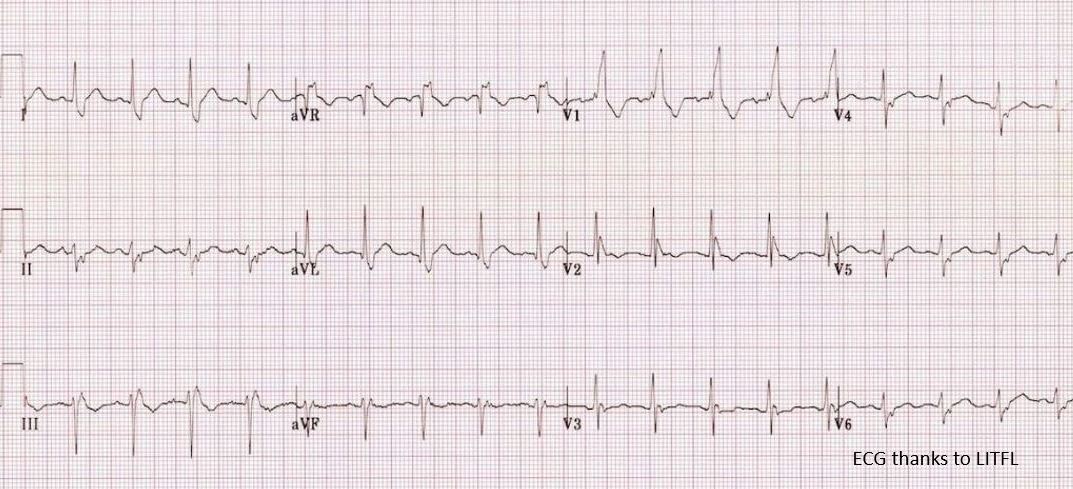
The ECG shows sinus tachycardia with a RBBB. Note the left axis deviation (voltage up in lead l, down in aVF) which is from a LAFB (Left anterior fasicular block).
So---a bifasicular block.
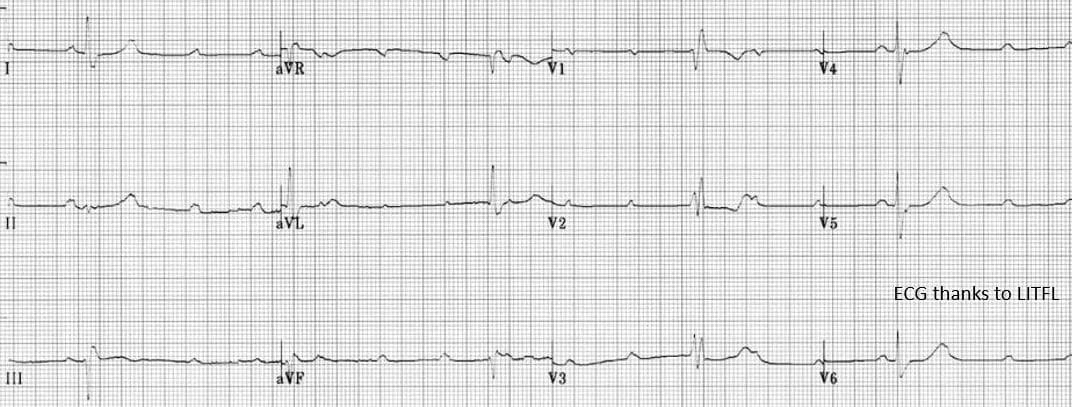
Another elderly patient presenting with syncope. What rhythm does the ECG show?
You would expect with such a slow heart rate that it would be a third degree heart block. However if you look closely the Ps and QRSs are not dissociated. It is in fact Mobitz type 2 that required a temporary then permanent pacemaker.
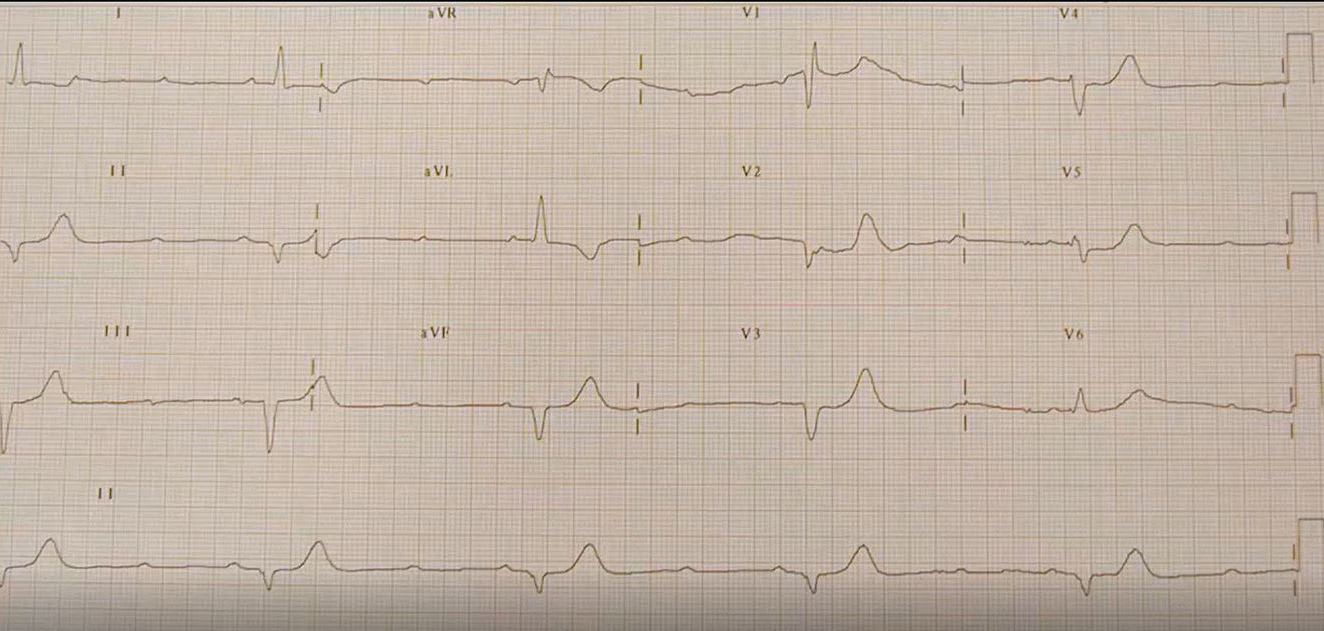
A 64yr old man presented to ED following a syncope. The following ECG was performed. What does it show?
The tri bit is:
3rd degree heart block
RBBB
LAHB (Left axis deviation)
This is the preserved heart of a blue whale. It weighs 199.5kgs. How many litres did it pump per heart beat?

For terrestial animals the elephant has the biggest heart. The world's smallest heart is the fairyfly---a tiny wasp <2mm long.