Shoulders and clavicle injuries.

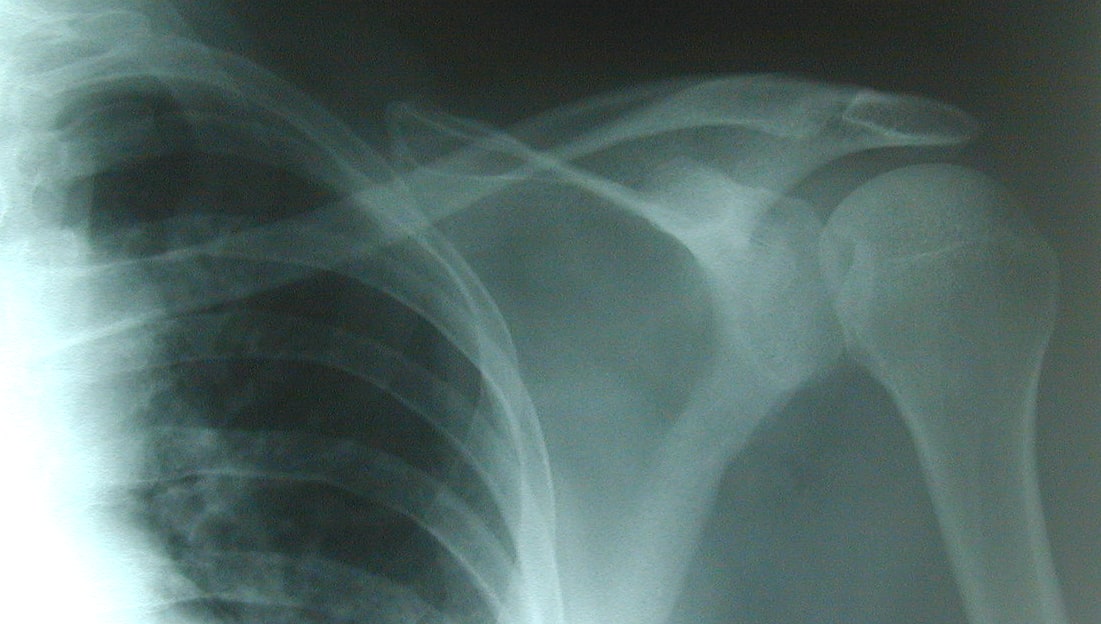
What does this picture show?

Acromioclavicular joint dislocations are graded 1 to 6 but we usually see the first 3.
Grade 1--Clavicle is not elevated. (Mild sprain of the acromiovlavicular lig).
Grade 2 Clavicle is elevated but not above the superior border of the acromium (rupture of the ac lig and sprain of the corococlavicular lig).
Grade 3--Clavicle is above the superior border of the acromium. (Both ac and cc ligaments ruptured).
This skateboarder fractured his clavicle. What mechanism generally does this?
The fall on the outstretched arm transmits the force upwards along the extended arm. The mid shaft of the clavicle, which is a comparatively weak area, takes the impact and fractures.
What is importance of the area noted in this picture?

The so called "Regimental Badge" area is the sensory area supplied by the Axillary nerve. It needs to be checked before and after relocations of the shoulder.
What does this image show?

The injury can occur with anterior shoulder dislocations. The anteroinferior aspect of the labrum is broken off from the glenoid. If I had one after an anterior shoulder dislocation I would get further imaging (CT or MRI) and see a shoulder surgeon.
Mel Gibson used a "non recognised" technique to relocate his shoulder. Which of the below techniques is also not recognised?
The Hippocratic technique is well recognised but used rarely in Australian Emergency Departments now. The Hippathetic is made up and even sounds iffy. Mel Gibson would probably have just fractured his humerus if he tried smashing it like he did in the Lethal Weapon 2 movie.
This is an AP of a posterior shoulder dislocation. Which is the following is not a sign you can look for?
The Trough sign is also known as the reverse Hill-Sachs sign. The light bulb sign is because the head in internal rotation looks like a light bulb. The piece of pizza sign is to do with lunate dislocations of the wrist.
This rugby player suffered an acromioclavicular injury. What mechanism generally causes these injuries?
It occurs by a very different mechanism to that of a fractured clavicle. The ac joint injury is a direct force whilst the fractured clavicle occurs as a transmitted force from an outstretched arm (ask any road cyclist).
What do we call this type of shoulder dislocation?

This is the rare inferior shoulder dislocation or "Luxatio erecta" which means to place upwards. Incidentally "Dolet brachium" means painful arm and "Infelicis" translates to unlucky. Personally I like "Question in class".
What do we call this manoeuvre of reducing a dislocated anterior shoulder dislocation without sedation?
Described by the Kiwi Emergency Physician Neil Cunningham. And it does have the advantage that you do not require a bed to relocate the shoulder.
What are these medical and nursing staff trying to do?

Relocation of posterior shoulder dislocations need deep sedation, traction and often physically pushing the humeral head from behind.